Union Safety Reps have known ever since the staart of the Coronavirus pandemic that the virus is airborne and that is the main way the virus is spread. It follows too, that as a result it is easilly passed on to those breathing in the same air source containing the contaminant.
Despite this, the Government and it's agencies weree very slow indeed in recognising this and promoting mitergation in the form of appropriaate risk assessment, looking at or modifying airconditioning and ventilation systems; and even in ensuring the public and workers are protacted by wearing suitable facemasks.
With new information now being available, the CWU has previouslty issued advice to their members via letters to branches, the most recent of which is LTB566/21 containing details of sources of iunformation and best practice in mitigating the Coronavirus in workplaces and in the public arena.
 The CWU National Health, Safety, and Environment Officer; Dave Joyce's letter to branches entitled 'Covid-19 Guide On Ventilation And CO2 Monitoring To Help Combat Airborne Covid-19 Transmissions' provides key advice and resources and is in part reproduced below:
The CWU National Health, Safety, and Environment Officer; Dave Joyce's letter to branches entitled 'Covid-19 Guide On Ventilation And CO2 Monitoring To Help Combat Airborne Covid-19 Transmissions' provides key advice and resources and is in part reproduced below:
The main way in which people are infected with the Covid-19 virus is through inhalation of air carrying very small fine droplets and aerosol particles that contain infectious virus. Risk of transmission is greatest within indoor, stuffy, poorly ventilated, crowded rooms, spending long periods near an infected person where the concentration of these very fine droplets and particles is greatest and the air is not being changed.
People release very fine respiratory fluid droplets and aerosol particles during exhalation. The smallest of these fine droplets are small enough to remain suspended in the air for minutes to hours if ventilation is not changing the air and can carry virus and transmit infection if inhaled by another person.
There is robust evidence supporting the significance of airborne aerosols in the transmission of the Covid-19 virus. Implementing effective ventilation systems reduces airborne transmission of Covid-19 aerosols.
Employers must adopt strategies to ensure sufficient ventilation rates and to avoid simple recirculation of air in workplaces.
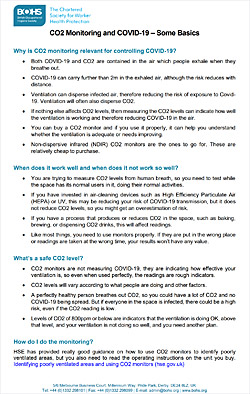
Carbon dioxide (CO2) sensors can be used as indicators of the build-up of exhaled air and serve as a simple way to monitor and optimize ventilation. Most CO2 monitors are the Non-dispersive Infrared (NDIR) type, and these are the ones that should be used. The aim is to measure CO2 levels from human breath, so testing should be done when the space has its normal users in it, doing their normal activities, and not when areas are empty or underpopulated.
The British Occupational Hygiene Society (BOHS) has published very simple guidance on CO2 monitors (copy available from the Unionsafety E-Library).
Assuring a minimum ventilation rate of 4 to 6 air changes per hour (ACH) and maintaining carbon dioxide levels below 700 to 800 ppm is advised, although the ventilation type and airflow direction and pattern should also be taken into account.
The World Health Organisation also recommends ventilation rates of 8-12 litres per second per person (l/s/p). The World Health Organisation has set out a “Roadmap to improve and ensure good indoor ventilation in the context of Covid-19” and this is available at the following link: https://www.who.int/publications/i/item/9789240021280
HSE Advice
The UK Government has provided guidance available at: https://www.gov.uk/guidance/working-safely-during-covid-19/offices-factories-and-labs#offices-3-1 on ventilation and the use of CO2 monitors, pointing to HSE advice (copy attached). This includes: ‘Identifying poorly ventilated areas and using CO2 monitors’.
Risk Assessment
The priority is risk assessments to identify areas of the workplace that are usually occupied and poorly ventilated, prioritising these areas for improvement to reduce the risk of aerosol virus transmission.
There are some simple ways to identify poorly ventilated areas:
- Look for areas where people work and where there is no mechanical ventilation or natural ventilation such as open windows, doors, or vents.
- Check that mechanical systems provide outdoor air, temperature control, or both. If a system only recirculates air and has no outdoor air supply, the area is likely to
be poorly ventilated.
- Identify areas that feel stuffy or smell bad.
- Use carbon dioxide (CO2) monitors. People exhale carbon dioxide (CO2) when they breathe out. If there is a build-up of CO2 in an area, it can indicate that ventilation needs improving. Although CO2 levels are not a direct measure of possible exposure to COVID-19, checking levels using a monitor can help you identify poorly ventilated areas.
- Take multiple measurements in occupied areas to identify a suitable sampling location to give a representative measurement for the space. In larger spaces it islikely that more than one sampling location will be required.
 Take measurements at key times throughout the working day and for a minimum of one full working day to ensure the readings represent normal use and occupancy.
Take measurements at key times throughout the working day and for a minimum of one full working day to ensure the readings represent normal use and occupancy.
- Recording CO2 readings, number of occupants, the type of ventilation in operation, and the time and the date will help to decide if an area is poorly ventilated.
- CO2 measurements should be used as a broad guide to ventilation within a space rather than treating them as ’safe thresholds’. Outdoor levels are around 400ppm and indoors a consistent CO2 value less than 800ppm is likely to indicate that a space is well ventilated. An average of 1500ppm CO2 concentration over the occupied period in a space is an indicator of poor ventilation.
Action should be taken to improve ventilation where CO2 readings are consistently higher than 1500ppm.Where there is continuous high levels of physical activity (such as dancing, sport or exercising), providing ventilation sufficient to keep CO2 levels below 800ppm is recommended.
- Face Masks, a mitigation put in place to address droplet transmission, is also effective in reducing the chances of aerosol inhalation because aerosol concentrations are
much higher in close proximity to an infected individual.
- The WHO, and public health agencies, still recommend maintaining physical distancing where it is possible as another mitigation. However, distancing is not always sufficient to protect against aerosols that travel a significant range. Airborne transmission of Covid-19 occurs in poorly ventilated rooms when occupants inhale infectious room air.
Ventilation and Aerosols
- Additionally, although distancing helps by moving people away from the most concentrated parts of respiratory plumes, distancing alone does not stop transmission and is not sufficient without other measures, such as ventilation. The number of people emitting infectious aerosols, and the amount of time spent in enclosed spaces and the unknown number of asymptomatic infected individuals present in specific environmental settings is an additional challenge in respiratory disease control. Engineering measures to reduce aerosol concentrations through ventilation, disinfection, masks etc., remain critical to reducing airborne transmission risks.
- It is absolutely clear that airborne transmission is a major pathway for the spread of Covid-19. It is worth noting that measures to improve indoor air quality will lead to health benefits extending well beyond the Covid-19 pandemic.
Use of Air Cleaning and Filtration Units
- Air cleaning and filtration units which employ either high efficiency particulate air (HEPA) filters or ultraviolet-based devices are also advocated by some organisations to help remove viruses and other pathogens and allergens from the air.
However, they are not a substitute for ventilation and the HSE has been clear that employers should prioritise any areas identified as poorly ventilated for improvement in other ways before considering using an air cleaning device. Therefore, they should only be used in addition to, not instead of, adequate ventilation. Testing is still being done on filtration and UV devices. The UK Government has announced it is conducting a trial of filtration units in schools, but this is not expected to report until 2022.
Action for Reps
Below are some standards that Safety Reps will find useful when discussing this matter with management. Seek to agree these standards for ventilation rates:
– A minimum ventilation rate of 4 to 6 air changes per hour, or
– Maintaining CO2 levels below 700 to 800 ppm, or
– Ventilation rates of 8-12 litres per second per person (l/s/p).
Note: The Health, Safety & Environment Department has raised the issue of providing CO2 monitors and improved ventilation and space standards in the RMG and POL Buildings Estates.)
Further Information:
World Health Organisation “Roadmap to improve and ensure good indoor ventilation in the context of Covid-19” March 2021 https://www.who.int/publications/i/item/9789240021280
UK government guidance
https://www.gov.uk/guidance/working-safely-during-covid-19/offices-factories-and-labs#offices-3-1
HSE guidance
https://www.hse.gov.uk/coronavirus/equipment-and-machinery/air-conditioning-and-ventilation/assesssment-of-fresh-air.htm
HSE-using-co2-monitors-to-identify-poor-ventilation
CIBSE (Chartered Institution of Building Services Engineers)
https://www.cibse.org/news-and-policy/august-2021/new-air-cleaning-guidance-for-reducing-covid-19-sp
BESA (Building Engineers Services Association) and REHVA (Federation of European Heating Ventilation and Air Conditioning)
https://www.thebesa.com/media/837805/besa-guidance-covid-19-practical-measures-for-building-services-operation.pdf
BOHS (British Occupational Hygiene Society)
https://www.bohs.org/app/uploads/2021/09/CO2-Monitoring-and-Covid-19-Some-Basics.pdf
Source: CWU
See also: unionsafety e-library for above and additional documentation and guidance.

